Fibrous dysplasia
Introduction
- A benign fibro-osseous lesion of immature mesenchymal cells.
- Commonly affects long bones, ribs, and skull.
Pathophysiology
- Originates from mutated pluripotent embryonic cells leading to skeletal stem cells.
- Lesions form as cancellous bone is replaced with fibrous tissue and immature woven bone.
- Monostotic FD (70% of cases) vs. Polyostotic FD.
Genetic Basis and Related Syndromes
- Genetic mutation: Chromosome 20q13 at the GNAS1 locus.
- Constitutively active mutant of the α subunit of the G protein (Gsα).
- McCune-Albright syndrome: Characterized by polyostotic FD, endocrinopathy, café au lait spots.
Clinical Presentation
- Monostotic FD usually presents by age 30.
- Polyostotic FD presents in early childhood.
- Symptoms: Painless osseous expansion, facial asymmetry.
- Craniofacial involvement: Ethmoid (71%), Sphenoid (43%), Frontal (33%), etc.
Diagnosis
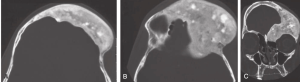
- MRI: For cranial nerve compression.
- Histology: “Chinese figure” formation in bone trabeculae.

Treatment
- Asymptomatic lesions: Conservative management.
- Medications: Alendronate (bone density), Denosumab (reduces pain but concerns over side effects).
- Surgical options: Contouring, total resection, computer-based planning, timing for children.
Considerations
- McCune-Albright syndrome management.
- Orbital apex involvement: Proptosis, diplopia, and options for optic nerve compression.
- Malignant transformation: Rare (0.4 to 4%).